Author Archives: Instep
Author Archives: Instep
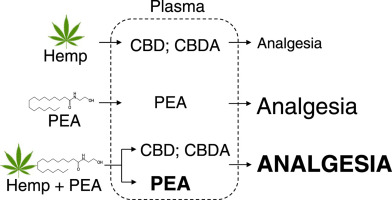
This Study (Click Here for full text) in mice from the National Academy of Science, Engineering and Medicine (NASEM) in Washington DC – showed that the combination of the two products produced a synergetic effect greater than low doses of either.
In pharmacokinetic tests (which describe the distribution, absorption, breakdown and excretion of compounds) – showed that the use of the two substances prolonged the possible beneficial effects of both PEA and HOE/CBD for the treatment of acute and chronic pain.
In Australia, you need to see your doctor for access to most CBD products. This may change in the future, particularly with low-THC versions.
PEA, which is a fatty acid found in most mammalian cells and in a variety of different foods including human breast milk and lecithin has been studied for many decades. You can find many studies that show that PEA can assist with pain and inflammation, and has a very good safety profile. (And PEA is NOT psycho-active or addictive.)
PEA is available (without a prescription) here. It is available in PEA Capsules (gelatin and vegetable) and PEA skin cream in two different strengths. PEA is also an prized ingredient in high-end anti-aging skin care products.
Be sure to check with your health care professional if you have any questions about any aspect of the use of PEA.

doi: 10.1007/s10787-019-00582-9. Epub 2019 Mar 29.
Background: The aim of the study was to assess the safety, tolerability and efficacy of palmitoylethanolamide (PEA) when dosed at 300 mg and 600 mg per day on symptoms of knee osteoarthritis.
Methods: This was a single site, comparative, double-blind placebo controlled study in adults with mild to moderate knee osteoarthritis with 111 participants randomized to receive 300 mg PEA, 600 mg PEA or placebo each day, in divided doses b.i.d, for 8 weeks. The primary outcome was the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). The secondary outcomes were the Numerical Rating Scales (NRS) for pain, the Depression Anxiety Stress Scale (DASS), the Perceived Stress Scale (PSS), the Pittsburg Sleep Quality Index (PSQI), the Short Form Health Survey (SF-36), the use of rescue pain medication and clinical safety assessment.
Results: There was a significant reduction in the total WOMAC score in the 300 mg PEA (p = 0.0372) and the 600 mg PEA (p = 0.0012) groups, the WOMAC pain score (300 mg PEA, p = 0.0074; 600 mg PEA, p = < 0.001), the WOMAC stiffness score (PEA 300 mg, p < 0.0490; 600 mg PEA, p = 0.001) and in the WOMAC function score in the 600 mg PEA group (p = 0.033) compared to placebo. The NRS pain evaluations for “worst pain” and “least pain” were significantly reduced in the 300 mg PEA group (p < 0.001, p = 0.005) and the 600 mg PEA group (p < 0.001, p < 0.001) compared to placebo. There was a significant reduction in anxiety (DASS) in both active treatment groups (300 mg PEA, p = 0.042; 600 mg PEA group (p = 0.043) compared to placebo. There were no changes in the clinical markers and the product was well tolerated.
Conclusions: The study demonstrated that palmitoylethanolamide may be a novel treatment for attenuating pain and reducing other associated symptoms of knee osteoarthritis. Further studies on the pharmacological basis of this anti-inflammatory effect are now required.
Keywords: Inflammation; N-acylethanolamines; Osteoarthritis; Pain; Palmitoylethanolamide.
 20% OFF Valentine's Day SALE")
Palmitoylethanolamide has been shown to reduce pain and inflammation. Make this your best Valentine’s Day ever, crank up the ROMANCE. And here is 20% of PEA to help…

Here are the highlights of the excellent review paper.

This Australia Day Weekend, help yourself. $10 off PEA 120 capsule bottles (300mg).
Use TRIAL code in the coupon box on checkout. https://palmitoylethanolamide.com.au/shop/
Applies to both vegetable and gelatin capsules. Max order is 12 bottles.
Expires midnight on Monday.
Aim of the study was to evaluate the effectiveness of micronized palmitoylethanolamide (PEA)-transpolydatin in the treatment of chronic pelvic pain in women affected by endometriosis.
Twenty-four patients with suspected endometriosis affected by severe pelvic pain were enrolled. All patients received two tablets a day of PEA 400 mg and 40 mg polydatin for 90 days consecutively. A Visual Analogic Scale was used for the assessment of the severity of global pain, dysmenorrhea, dyspareunia, dysuria and dischezia. A second questionnaire was submitted to patients to assess the quality of life. The compilation of a diary lead us to evaluate the monthly assumption of any painkillers. Patients were evaluated at the begin of the treatment and then monthly until the end of the study (90 days). The statistical analysis was performed by using the ANOVA for the analysis of variance.
Statistically significant results were found in relation to pelvic pain, dysmenorrhea and dyspareunia compared to the initial evaluation of patients. Results related to dysuria and dischezia were not statistically significant (P>0.05). The decrease in pelvic pain leads to an improvement of the quality of life of patients. A decreased assumption of nonsteroidal anti-inflammatory drugs (NSAIDs) was also observed.
PEA could be considered an effective supplement to conventional analgesic therapies in the management of pelvic pain related to endometriosis.
Endometriosis is a chronic oestrogen-dependent gynaecological disorder, the most common symptom of which is pain. Inflammation can be considered one of the major causes of pain in endometriosis. In particular, degranulating mast cells have been found in significantly greater quantities in endometriotic lesions than in unaffected tissues. The increase in activated and degranulating mast cells is closely associated with nerve structures in painful endometriotic lesions. These observations indicate that inflammation due to mast cells may contribute to the development of pain and hyperalgesia in endometriosis. Controlling mast-cell activation may therefore relieve the pain associated with endometriotic lesions.
Four patients presenting an endometriosis-related pain intensity >or=5 (visual analogue scale for pain, or VAS) were enrolled and monitored during 3 months of the following treatment: oral palmitoylethanolamide 400mg and polydatin 40mg, twice daily for 90 days. Deep dyspareunia, dyschezia, dysuria, dysmenorrhoea and analgesic drug use during the 3-month follow-up period were also monitored, with the aim of demonstrating a reliable reduction in chronic pelvic pain.
The preliminary results indicate that all patients enrolled experienced pain relief as early as 1 month after starting treatment. Furthermore, a reduction in the analgesic drugs usually employed for pain control was observed in all subjects treated. Additionally, some improvements in endometriotic lesions seemed to be demonstrated by imaging.
The palmitoylethanolamide-polydatin combination seems to be very useful in controlling chronic pelvic pain associated with endometriosis. As a result of these findings we have initiated a multi-centre pilot study to verify the effectiveness of this treatment in controlling the chronic pelvic pain associated with endometriosis.
Effect of ultramicronized-palmitoylethanolamide and co-micronized palmitoylethanolamide/polydatin on chronic pelvic pain and quality of life in endometriosis patients: An open-label pilot study
Received 6 February 2019
Accepted for publication 12 July 2019
Published 12 August 2019 Volume 2019:11 Pages 443—449
DOI https://doi.org/10.2147/IJWH.S204275
Checked for plagiarism Yes
Review by Single-blind
Peer reviewer comments 2
Editor who approved publication: Professor Everett Magann
1Division of Gynecology and Obstetrics, Department of Surgical Sciences, University of Cagliari, Cagliari, Italy; 2Division of Gynecology and Obstetric, Hospital San Francesco, Nuoro, Italy; 32nd University Department of Obstetrics and Gynecology, Hippokratio General Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece
Purpose: The aim of the present study was to evaluate the effectiveness of the ultramicronized-palmitoylethanolamide (um-PEA) and co-micronised palmitoylethanolamide/polydatin m(PEA/PLD) in the management of chronic pelvic pain related to endometriosis in patients desiring pregnancy.
Patients and methods: Thirty symptomatic women with laparoscopic diagnosis of endometriosis and pregnancy desire were enrolled. Patients were treated with um-PEA twice daily for 10 days followed by m(PEA/PLD) twice daily for 80 days. Intensity of chronic pelvic pain, dyspareunia, dysmenorrhea, dyschezia, and dysuria were evaluated at baseline, after 10, 30, 60, 90 days and after 30 days from the end of treatment, by VAS. Quality of life and women’s psychological well-being were evaluated at baseline and at the end of the treatment after 90 days with 36-Item Short Form Health Survey questionnaire and Symptom Check list-90 questionnaire, respectively. All collected data were analyzed with the non-parametric Wilcoxon test.
Results: At the end of the treatment, all patients showed a significant improvement in chronic pelvic pain, deep dyspareunia, dysmenorrhea, dyschezia, as well as in quality of life and psychological well-being.
Conclusion: In spite of the study’s limited sample size and the open-label design, this research suggests the efficacy of um-PEA and m(PEA/PLD) in reducing painful symptomatology and improving quality of life as well as psychological well-being in patients suffering from endometriosis. Additionally, this treatment did not show any serious side effect, proving particularly suitable for women with pregnancy desire and without other infertility factors.
Keywords: endometriosis, chronic pelvic pain, psychological well-being, quality of life, ultramicronized-palmitoylethanolamide, co-micronized palmitoylethanolamide and polydatin
Source: https://www.dovepress.com/effect-of-ultramicronized-palmitoylethanolamide-and-co-micronized-palm-peer-reviewed-article-IJWH

Why this matters
Study design
Key results
Limitations
https://www.univadis.co.uk/viewarticle/palmitoylethanolamide-shows-benefit-in-knee-osteoarthritis-664187
Osteoarthritis (OA) is a common progressive joint disease in dogs and cats. The goal of OA treatment is to reduce inflammation, minimize pain, and maintain joint function. Currently, non-steroidal anti-inflammatory drugs (e.g., meloxicam) are the cornerstone of treatment for OA pain, but side effects with long-term use pose important challenges to veterinary practitioners when dealing with OA pain. Palmitoylethanolamide (PEA) is a naturally-occurring fatty acid amide, locally produced on demand by tissues in response to stress. PEA endogenous levels change during inflammatory and painful conditions, including OA, i.e., they are typically increased during acute conditions and decreased in chronic inflammation. Systemic treatment with PEA has anti-inflammatory and pain-relieving effects in several disorders, yet data are lacking in OA. Here we tested a new composite, i.e., PEA co-ultramicronized with the natural antioxidant quercetin (PEA-Q), administered orally in two different rat models of inflammatory and OA pain, namely carrageenan paw oedema and sodium monoiodoacetate (MIA)-induced OA. Oral treatment with meloxicam was used as benchmark.
The present findings shed new light on some of the inflammatory and nociceptive pathways and mediators targeted by PEA-Q and confirm its anti-inflammatory and pain-relieving effects in rodent OA pain models. The translatability of these observations to canine and feline OA pain is currently under investigation.
PEA-Q is a novel co-ultramicronized formulation of PEA and quercetin whose effects were investigated in two pre-clinical models of OA pain in rats. Oral administration of PEA-Q decreased pain sensitivity, improved locomotor function, reduced inflammatory signs and mediators and lowered histological damage score. Although the underlying mechanism(s) of the observed effects are beyond the scope of our study, the particular cellular targets of PEA (e.g., mast cells and microglia) [19], redundancy of its receptors (direct and direct agonism on nuclear and membrane cannabinoid receptors) [14] and oxidative stress addressed by quercetin [22, 37] comprise targets that could be different from standard pharmacological tools (i.e., NSAIDs). Importantly, toxicological studies show that micronized and ultramicronized PEA is safe, the LD50 being greater than 2000 mg/kg [53]. Individually or in association with different antioxidant polyphenols, micronized and ultramicronized PEA has a long track record of use in human and veterinary patients, with good-to-excellent tolerability [14]. Moreover, prolonged use of PEA is not associated with the development of tolerance [43, 54]. There is an unmet need in veterinary medicine for the development of new agents to treat OA-associated pain which target alternative mechanisms distinct from currently approved drugs. The collective observations presented here propose that PEA-Q shows promise for multimodal pain management in canine and feline OA.”
Full Study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5541643/
The information provided on this page is for educational and informational purposes only. The information provided is not, nor is it intended to be, a substitute for professional advice or care. Please seek the advice of a qualified health care professional in the event something you have read here raises questions or concerns regarding your health.
No claims are made here about benefits of PEA in any medical condition, as PEA (not a prescription item) is governed by TGA in Australia. Research is shown for readers education only.

Accepted for publication 17 September 2015
“PEA has been tested in a variety of animal models for nerve compression and has been evaluated in eight different clinical trials in total, in 1,366 patients with nerve compression syndromes. Both the preclinical as well as the clinical results point in the same direction: PEA acts as a safe analgesic compound in nerve compression. Its safety and efficacy profile supports the clinical use of PEA in compression syndromes such as sciatic pain and carpal tunnel syndrome. PEA is easy to administer. The NNT of PEA for sciatic pain to reach 50% pain reduction is 1.5 and the number needed to harm is at least in the hundreds, but for the time being not calculable due to the absence of serious and troublesome side effects leading to dropouts in clinical trials. The risk–benefit balance of PEA therefore favors its inclusion in the therapeutic armamentarium of chronic pain. PEA can be administered both as a stand-alone analgesic as well as part of a multimodal therapy regime.” [NNT ratio: Number Needed to Treat: The ideal NNT is 1, where everyone improves with treatment and no one improves with control. A higher NNT indicates that treatment is less effective. NNT is similar to number needed to harm (NNH), where NNT usually refers to a therapeutic intervention and NNH to a detrimental effect or risk factor.]
Here is a good summary article about PEA that talks about chronic pain conditions and it’s use. https://www.fxmedicine.com.au/blog-post/pea-pain Summary:
The information provided on this page is for educational and informational purposes only. The information provided is not, nor is it intended to be, a substitute for professional advice or care. Please seek the advice of a qualified health care professional in the event something you have read here raises questions or concerns regarding your health.

Palmitoylethanolamide (PEA), an endogenous fatty acid amide, has been demonstrated to bind to a receptor in the cell nucleus – the peroxisome proliferator–activated receptor – and performs a great variety of biological functions related to chronic and neuropathic pain and inflammation, as has been demonstrated in clinical trials. These include peripheral neuropathies such as diabetic neuropathy, chemotherapy-induced peripheral neuropathy, carpal tunnel syndrome, sciatic pain, osteoarthritis, low-back pain, failed back surgery syndrome, dental pains, neuropathic pain in stroke and multiple sclerosis, chronic pelvic pain, postherpetic neuralgia, and vaginal pains. Probably due to the fact that PEA is an endogenous modulator as well as a compound in food, such as eggs and milk, no serious side effects have been reported, nor have drug–drug interactions. This article presents a case series describing the application and potential efficacy and safety of PEA in the treatment of various syndromes associated with chronic pain that is poorly responsive to standard therapies.
Extract:
”
Chemotherapy-induced neuropathic pain (patient 1) must be taken into account for both the associated disability and distress, but also to optimize the chemotherapy itself. Recently, the effect of PEA on pain and nerve functions in patients with chemotherapy-induced painful neuropathy was assessed.26 In brief, 20 patients undergoing thalidomide plus bortezomib treatment for multiple myeloma received 300 mg PEA twice daily for 2 months, starting after chemotherapy-induced neurotoxicity was established. Although no variable returned to normal, pain and all neurophysiological measures – assessing Aα, Aβ, and Aδ fibers – significantly improved. These results suggest a possible neuroprotective effect of PEA on myelinated nerve fibers. Importantly, concomitant PEA treatment allowed the maintenance of chemotherapeutic dose without further deterioration of nerve functions. The ability to continue chemotherapy in patients suffering from neuropathic pain, instead of stopping or reducing therapy, would clearly impact positively on survival rates also. A multicenter double-blind study evaluating the efficacy and safety of PEA in chemotherapy-induced neuropathic pain is currently in progress.
PEA represents a promising addition to our therapeutic armamentarium for neuropathic pain, with potential for good tolerability and a low propensity for side effects.
Full Article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3500919/
The present study evaluated the effectiveness of micronized palmitoylethanolamide (PEA-m) treatment in reducing the painful symptoms experienced by diabetic patients with peripheral neuropathy. PEA-m, a fatty acid amide of the N-acylethanolamine family, was administered (300 mg twice daily) to 30 diabetic patients suffering from painful diabetic neuropathy. Before treatment start, after 30 and 60 days the following parameters were assessed: painful symptoms of diabetic peripheral neuropathy using the Michigan Neuropathy Screening instrument; intensity of symptoms characteristic of diabetic neuropathic pain by the Total Symptom Score; and intensity of different subcategories of neuropathic pain by the Neuropathic Pain Symptoms Inventory. Hematological and blood chemistry tests to evaluate metabolic control and safety were also performed. Statistical analysis (ANOVA) indicated a highly significant reduction in pain severity (P < 0.0001) and related symptoms (P < 0.0001) evaluated by Michigan Neuropathy Screening instrument, Total Symptom Score, and Neuropathic Pain Symptoms Inventory. Hematological and urine analyses did not reveal any alterations associated with PEA-m treatment, and no serious adverse events were reported.
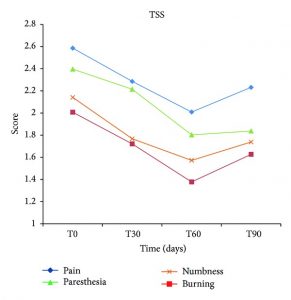
These results suggest that PEA-m could be considered as a promising and well-tolerated new treatment for symptomatology experienced by diabetic patients suffering from peripheral neuropathy.
Effect of micronized PEA on each single neuropathic pain symptom assessed by Total Symptom Score (TSS). The intensity and frequency of pain, burning, paresthesia, and numbness, evaluated by TSS, show a significant mitigation (P < 0.0001) after 60 days of treatment compared to baseline. This effect persists even one month after treatment discontinuation.
Full Study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3996286/
The information provided on this page is for educational and informational purposes only. The information provided is not, nor is it intended to be, a substitute for professional advice or care. Please seek the advice of a qualified health care professional in the event something you have read here raises questions or concerns regarding your health.
No claims are made here about benefits of PEA supplement in any medical condition, as PEA (not a prescription item) is governed by TGA in Australia. Research is shown for readers education only.


 2,5
2,5